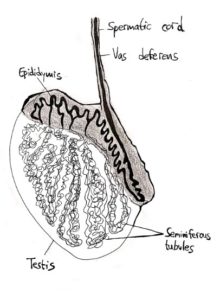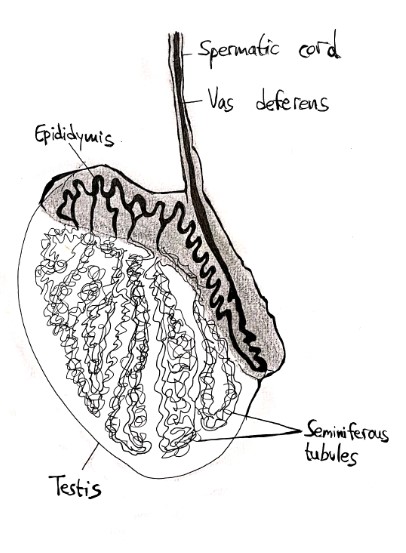
Obstructive azoospermia (OA) occurs when something blocks the mature sperm’s ability to reach the ejaculate. Instead, they remain “stuck” in the testis. Several surgical techniques have been developed in order to reach and extract these cells, which can then be used for IVF. In cases of non-obstructive azoospermia (NOA), when a male has no sperm cells in the ejaculate however no evidence of a blockage can be found, similar techniques of sperm retrieval are used in order to find sperm directly in the testis.
Microsurgical Epididymal Sperm Aspiration (MESA)
This method is used for men who have an epididymal obstruction preventing the sperm from moving, as well as for men who have undergone a vasectomy or who have CBAVD (link). During MESA, an incision is made in the scrotum while under local anesthesia. The fluid is then aspirated from the epididymis and analyzed under the microscope for sperm cells. This method can be advantageous in cases of OA, as it can retrieve a large amount of high quality, motile sperm cells. These retrieved cells will usually be frozen for future use.
Testicular Sperm Aspiration (TESA), also known as Testicular Fine Need Aspiration (TEFNA)
TESA is performed under local anesthesia and is usually the method chosen for males with OA who are retrieving sperm for IVF/ICSI. The timing of the procedure will usually be coordinated with their female partner’s ovulation, occurring on the same day as her egg retrieval. TESA uses a needle, inserted into the testicle, to aspirate tissue into a syringe. The tissue is then analyzed for its sperm content and quality, and IVF can be directly performed.
While it is minimally invasive and simple, TESA is not the most efficient method of retrieval and may cause damage to the testicular tissue.
Testicular Sperm Extraction (TESE)
For conventional TESE, a random incision is made in the testis and a sample of tissue is removed and analyzed. After removing a section of these tubules, the tissue is examined and searched for sperm. When found, the sperm can either be frozen or used for immediate IVF.
While TESE can be used for males with OA, it is also utilized for those with NOA, in which case the success of the procedure is not guaranteed and is difficult to predict. However, it can also be utilized as a diagnostic tool in males with NOA. In these cases, the results of the conventional TESE procedure may serve as a step before continuing on to what is currently the most common, efficient, and recommended procedure, the micro-TESE.
Microdissection TESE (microTESE)
In a micro-TESE, a wide initial incision is made in the scrotum to expose the testis. The surgeon then searches the entire testis for those larger, opaque testicular tubules which can indicate the presence of sperm. If found, small biopsies are taken, specifically from these healthy-looking tubules. If all the tubules appear the same, then random biopsies are taken from all over the testis. As the samples are removed, they are sequentially examined for sperm cells. When sperm cells are found, the procedure is concluded. In cases where sperm is not found in the operating room, the samples will continue to be searched extensively in the lab as well. In either case, each biopsy is analyzed under a microscope to search for mature sperm cells.
Micro-Tese is minimally invasive and safe, with a higher success rate than conventional TESE. The procedure is performed under an operating microscope, which allows the surgeon to be certain not to disturb the testicular blood supply, and allows him/her to differentiate between “healthy” tubules and the rest. It allows the specific targeting of regions that are more likely to contain mature sperm. The procedure also has a lower complication rate than others.
Which Technique?
The goal of each procedure is to retrieve enough sperm cells for IVF while inflicting minimal trauma to the testes. Therefore, the choice of which procedure will be individualized to each patient. The most efficient method is micro-TESE and is often the routine choice when NOA is suspected. However, in some cases, a less invasive procedure may be enough. It is important to take all factors of one’s cause under consideration, as the best chance for retrieval will be the first procedure, due to the potential trauma caused to the testis.
Pre-Op Treatment
In some males with impaired sperm production, the condition can be partially attributed to hormone imbalance or deficiencies. For example, men with NOA will often have low testosterone levels as well as high levels of estradiol. Testosterone is an important player in sperm production. In some cases, hormone therapy used to increase testosterone levels has been shown to improve sperm production, increasing the chances of successful sperm retrieval. (Will discuss more on-page about Klinefelter’s, maybe have a link here?)