Male hypogonadotropic hypogonadism (HH) occurs as a consequence of hormonal dysfunction affecting the basic mechanics behind male sexual development. In these cases, the hormones needed to allow the testes to function are either completely absent or inadequate. Thus, this condition can affect the ability to produce sperm and testosterone. This kind of impaired testicular function is estimated to occur in 1:10,000 to 1:86,000 males.
HH can either be congenital (present from birth) or acquired later in life, and the symptoms will vary accordingly. Approximately ⅔ of congenital HH cases are diagnosed as Kallman syndrome and come together with a lack of the ability to smell. In the remaining ⅓ of cases, the direct cause of the condition is unknown.
Acquired HH, where the individual is not born with the condition, can be caused by lifestyle or other factors, including drugs and alcohol abuse, radiation, infection, and some diseases.
An HH diagnosis can be isolated using hormone testing, where low levels of testosterone, FSH, and LH hormones (gonadotropins) can be positive indications of the condition. Since these hormones are normally produced as a response to the release of yet another hormone, GnRH, their absence indicates its absence as well. MRI imaging is used for diagnosis as well and is particularly useful in defining the presence of Kallman syndrome.
HH can hit either pre or post-puberty. In pre-pubertal cases, the individual will be short, with smaller testes and penis, have a high pitched voice, low muscle mass, and infertility. It can be difficult to differentiate these HH cases from delayed puberty. A final diagnosis is therefore only given once these individuals turn 18 and “simple” delayed puberty can be ruled out.
Post-pubertal HH presents in males with normal height, testes and penis size, and voice. However, these individuals also present with hot flashes, infertility, erectile dysfunction, increased body fat, and a general lack of well-being.
Hypogonadotropic Hypogonadism and Infertility
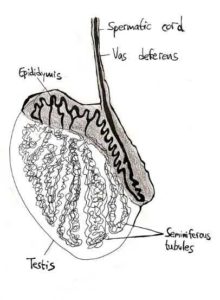
In Hypogonadotropic Hypogonadism, the testes do not receive the stimulation required to produce viable sperm. However, the fertility of these men is only reduced—imagine that all the required parts are present but are unable to communicate with one another as necessary. Therefore, HH represents a rare case where infertility may be reversible.
The therapy prescribed for HH will be dependent on the individual’s desire to achieve fertility. If the individual already has children or has no plans to have any, then a majority of the symptoms can be resolved through testosterone therapy. This treatment allows a normal sex life and preserves muscle and lean body mass, as well as results in positive changes in mood.
Where an individual still wishes to have children, GnRH, and/or gonadotropin hormone therapy is recommended to stimulate sperm production, which can take 6 months to 2 years. It is therefore advised to begin hormone therapy at least 6 months prior to attempting to conceive.
While these treatments do increase the total number of sperm, the number usually remains below normal levels. This does not negate spontaneous pregnancy. However, if a pregnancy does not occur after some time, it is recommended to try through assisted reproductive technologies such as IUI and IVF.